Hi everyone, Tim here. I’ve been in Montreal last week at the International Society of Autism Researchers (INSAR) annual conference. This conference brings autism researchers from around the world together to discuss and share the leading research into the autism spectrum.
Highlights from Day 3:
Transitioning into adulthood
Are healthcare providers ready to transition ASD teens to adulthood:
Lisa Croen discussed research into clinical providers in California and their ability to support teens transitioning into adulthood.
Sex differences in health outcomes:
Julie Taylor discussed sex differences in ASD health outcomes, particularly in transition time points.
So much Science and Research over the last 3 days!
Take home message:
Services are often underfunded in supporting ASD teens transitioning to adulthood, and this group is often underserved. Ongoing research is required to provide input to governments and service providers on best practice for transitioning teens.
Also while at INSAR I have discovered so many other great resources, which we have listed below.
Wonderful stories on going into hospital and what to expect for those who need some preparation. We will be adding this to our resource page for Hospital and Emergency!
This is an Australian website that has loads of links to Universities throughout Australia and NZ, as well as lots of programs and resources available (we have done the Secret Agent Society Training and would recommend!!)
Happy Days! We hope you enjoyed our reflections on the INSAR Conference 2019!!
INSAR Conference 2019 – Day 2
Hi everyone, Tim here. I’ve been in Montreal last week at the International Society of Autism Researchers (INSAR) annual conference. This conference brings autism researchers from around the world together to discuss and share the leading research into the autism spectrum.
Highlights from Day 2:
Multimodal Measurement of Sensory Processing
Measuring sensory reactivity reliably:
Teresa Tavassoli discussed the difficulties in accurately measuring sensory reactivity in autistic individuals.
I am part of Teresa’s team and you can find out more information here.
This is my poster! You can find a downloadable version here.
Lessons from psychophysical studies of somatic sensation in autism:
Carissa Cascio spoke about psychophysics, and in particular how tactile perception relates to ASD traits.
You can find our more about Carissa’s research here.
Neural habituation of sensory stimuli:
Shula Green described sensory over-responsivity and functional neuroimaging. She discussed differences in neural connectivity to touch and sound processing, particularly over time.
Relating abnormal tactile processing and cortical dysfunction in children with ASD:
Nick Puts continued the discussion on cortical differences in tactile processing in ASD individuals.
Take home message from these sessions:
The assessment of sensory reactivity in autistic individuals requires a multimodal approach that takes into consideration both questionnaire and observational methods. This should include measurement of perception (internal state) and not just reaction (external reaction).
Psychiatric Comorbidities
Adverse childhood experiences:
This talk by Amy Barrett highlighted the large percentage of ASD children who have adverse childhood experiences, including trauma, and how this is often overlooked in research and in clinical settings.
Paul Lipkin advised on his research on suicide behaviours in children and adolescents with autism and their access to medication and interventions. In particular, he looked at exploring factors contributing to suicidal behaviours.
Emotion dysregulation as a risk factor for suicide:
Caitlin Conner outlined her research and showed that increases in emotional dysregulation are correlated with higher reported suicidal ideation.
Depressed mood and interpretation of neuroscience data:
Katie Gotham spoke about how depressed mood in autism may obscure our interpretation of neuroscience research data. Analysing mood, anxiety and attention may help interpret research findings more accurately.
Group CBT for ASD and anxiety:
Audrey Blakeley-Smith presented on findings of a trial of group CBT for anxiety in a group of ASD teens with anxiety and intellectual disability.
Executive functioning:
Laura Anthony discussed an online executive functioning intervention – Unstuck. This online program allows for a self-paced, parent led intervention with tips and support.
Take home message:
Whilst research is making strides towards understanding psychopathology in autism, and in particular defining specific vulnerability profiles, there is still a lot to explore. Children with autism are also more likely to mask disorders like anxiety, or not be picked up by standard measures of psychopathology.
Hi everyone, Tim here. I’ve been in Montreal last week at the International Society of Autism Researchers (INSAR) annual conference. This conference brings autism researchers from around the world together to discuss and share the leading research into all aspects of the autism spectrum.
There were too many sessions and discussions to get to all of them, but I will be talking about the sessions that I was able to attend.
Highlights from Day 1
Autism and Mental Health
Autistic Burnout:
Discussion around Autistic people feeling overwhelmed by the sensory and social environment leading to burnout and meltdown. Christina Nicolaidis spoke about autistic burnout and its impact on adults. Currently there is little research into this area as a stand-alone phenomena in mental health.
You can find more about Christina’s research here.
ASD and Childhood Trauma:
This talk was about understanding specific indicators of traumatic reactions in autistic youth. Researchers (Connor Kerns et al.) are developing criteria to better understand and diagnose trauma, including PTSD, in children.
Dr Rachel Mosely spoke about self-injury without suicidality in autistic people. Her research looks at the why some autistic people injure without suicidal intent, and what predictors might help understand risk.
You can find out more about Dr Rachel and her research here.
Assessing suicidal behaviour:
Cecile Bardon spoke about how to engage people with ASD and intellectual disabilities to prevent suicide. In particular how to adapt services to meet those client’s needs.
Brenna Maddox described how her and her colleagues are investigating how to mitigate suicide risk in autistic individuals, including how to inform future clinical guidelines.
You can find out more about Brenna’s research here.
Suicide and ASD:
Anne Kirby discussed suicide in the autistic community. In particular, her research looks at the extent to which co-occuring mental health difficulties influence suicidality.
More information about Anne and her research can be found here.
Emotion regulation and therapeutic alliance in CBT:
Carly Aubaum spoke about how the therapeutic alliance can make CBT more accessible to autistic children, and enhance the therapy outcomes.
Emotion dysregulation in adolescents:
Virginia Carter Leno described research around the drivers of behaviours that challenge using physiological response measurements. She asked an important question; is it defiant behaviour or poor regulation strategies?
Problem behaviours, GI problems and Internalising symptoms:
Brad Ferguson is currently completing research into the link between gastrointestinal problems, behaviour and internalising symptoms in autistic individuals.
If you would like more information about Brad’s research you can find more here.
Anxiety in ASD and ID:
Breanna Winder-Patel discussed her research around understanding anxiety in children with ASD and an intellectual disability. In particular developing specific anxiety measures within the ASD population.
You can find out more here about Breanna’s projects and articles.
Quality of life:
Bethany Oakley spoke about how individual differences in QoL impacts on the development of mental health in autistic people.
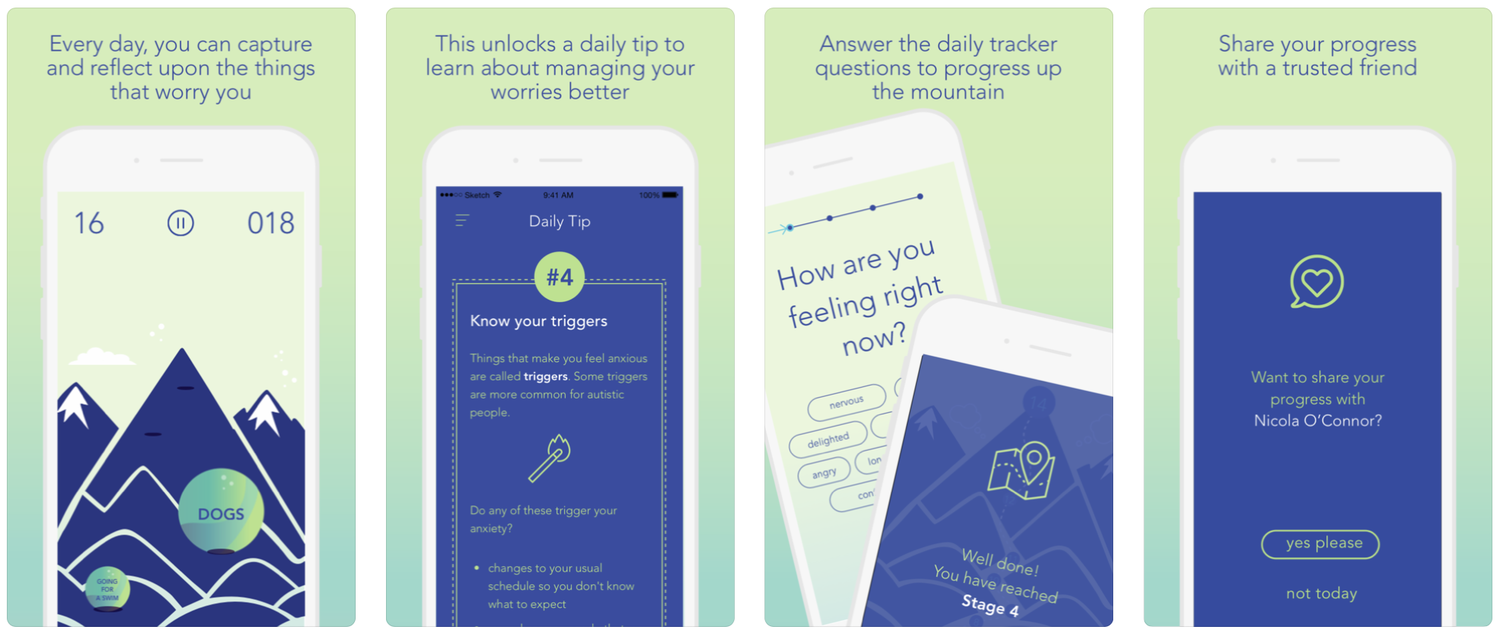
Molehill Mountain:
Sophie Carruthers presented on a new app to support autistic children and adults understand and manage anxiety and worries. The app is called “Molehill Mountain”.
Bullying can be defined as a subcategory of interpersonal aggression characterized by intentionality, repetition, and an imbalance of power, often with the element of abuse of power being a primary distinction between bullying and other forms of aggression (Smith & Morita, 1999; Vaillancourt, Hymel, & McDougall, 2003).
Bullying can include direct physical harm (physical bullying), verbal taunts and threats (verbal bullying), exclusion, humiliation, and rumour-spreading (relational or social bullying), and electronic harassment using texts, e-mails, or online mediums (cyberbullying).
Prevalence?
Prevalence rates for bullying vary, however research reveals that between 10% and 33% of school children are victimised, and 5% – 12% of children bully others (Cassidy, 2009; Kessel Schneider, O’Donnell, Stueve, & Coulter, 2012; Perkins, Craig, & Perkins, 2011).
Developmentally, peer bullying is evident as early as preschool, peaking during early high school, then declining towards the end of high school (Currie et al., 2012; Vaillancourt, Trinh, et al., 2010).
The World Health Organisation reports that overall peer victimisation has been decreasing over previous years (Currie et al., 2012), however cyber bullying is increasing (Jones, Mitchell, & Finkelhor, 2013). One reason put forward is that students are often aware of rules prohibiting physical harm to others, but find verbal and social bullying more difficult to identify (Hymel & Swearer, 2015).
Current Research:
Current research reveals that bullies are socially intelligent (Björkqvist, Österman, & Kaukiainen, 2000) and can have considerable status in their peer groups (Vaillancourt et al., 2003). As such, adults may be less able to recognize bullying perpetrated by students who appear to be socially competent, well-functioning individuals. Interventions should emphasise the interaction of individual vulnerabilities, context effects, and experiences with bullying and victimization. This includes understanding and addressing bullying as a systemic problem (Swearer & Hymel, 2015), and having schools implement school-wide, universal antibullying programs (Bradshaw, 2015).
Björkqvist, K., Österman, K., & Kaukiainen, A. (2000). Social intelligence – empathy = aggression? Aggression and Violent Behavior, 5, 191–200.
Bradshaw, C. P. (2015). Translating research to practice in bullying prevention. American Psychologist, 70, 322–332.
Cassidy, T. (2009). Bullying and victimisation in school children: The role of social identity, problem-solving style, and family and school context. Social Psychology of Education, 12, 63–76.
Currie, C., Zanotti, C., Morgan, A., Currie, D., DeLooze, M., Roberts, C., . . . Barnekow, V. (2012). Social determinants of health and well-being among young people. Health Behaviour in School-aged Children (HBSC) study: International report from the 2009/2010 survey. Health Policy for Children and Adolescents, No. 6. Copenhagen, Denmark: WHO Regional Office for Europe.
Hymel, S., & Swearer, S. M. (2015). Four decades of research on school bullying: An introduction.American Psychologist, 70(4), 293.
Jones, L. M., Mitchell, K. J., & Finkelhor, D. (2013). Online harassment in context: Trends from three youth internet safety surveys (2000, 2005, 2010). Psychology of Violence, 3, 53–69.
Kessel Schneider, S., O’Donnell, L., Stueve, A., & Coulter, R. W. C. (2012). Cyberbullying, school bullying, and psychological distress: A regional census of high school students. American Journal of Public Health, 102, 171–177.
Perkins, H. W., Craig, D. W., & Perkins, J. M. (2011). Using social norms to reduce bullying: A research intervention among adolescents in five middle schools. Group Processes & Intergroup Relations, 14, 703–722.
Smith, P. K., & Morita, Y. (1999). Introduction. In P. K. Smith, Y. Morita, J. JungerTas, D. Olweus, R. Catalano, & P. Slee (Eds.), The nature of school bullying: A cross-national perspective (pp. 1–4). London, UK: Routledge.
Swearer, S. M., & Hymel, S. (2015). Understanding the psychology of bullying: Moving toward a social-ecological diathesis–stress model. American Psychologist, 70, 344–353.
Vaillancourt, T., Hymel, S., & McDougall, P. (2003). Bullying is power: Implications for school-based intervention strategies. Journal of Applied School Psychology, 19, 157–176.
Vaillancourt, T., Trinh, V., McDougall, P., Duku, E., Cunningham, L., Cunningham, C.,…Short, K. (2010). Optimizing population screening of bullying in school-aged children. Journal of School Violence, 9, 233–250.
Visuals – why we love them (and the evidence)
VISUALS
This month the review of the evidence is all about our favourite resource in the world – VISUALS!!
RESEARCH
There is a large body of evidence linking cognitive and physical disabilities with externalising problematic behaviours (Visser et al., 2015; Artemyeva, 2016; Giltaij, Sterkenburg & Schuengel, 2015; Poppes et al., 2016).
In particular, the literature suggests that problematic behaviour in children with disabilities is related to deficits in receptive and expressive communication (Murphy, Faulkner & Farley, 2014; Ronen, 2001; Ketelaars et al., 2010; Conti-Ramsden & Botting, 2004).
Outcomes of problematic behaviour can include victimisation, development of poor peer relationships and long term difficulties with employment and romantic relationships (Murphy, Faulkner & Farley, 2014; Whitehouse et al., 2009).
As such, it is imperative to develop augmentative and alternative communication techniques to increase engagement in, and outcomes of, communication.
A review of the available literature shows the efficacy of using icons and pictures to aid in communication for children with additional needs (Flippin, Reszka & Watson, 2010; Hartley & Allen, 2015), particularly in the effectiveness of visual aids over text and words (Dewan, 2015).
Pooley and Berg (2012) report that “simple graphics can be rapidly communicated, processed and transmitted within a large and culturally diverse constituency” (p.361), and as such icons have the ability to be utilised across multiple domains.
Pictorial devices are already being used in classrooms, and there is good evidence for the effectiveness of these systems, such as PECS, in schools (Flippin, Reszka & Watson, 2010; Lerna et al., 2012).
In addition to this, augmentative and alternative communication for children with additional needs, including the use of visual aids, has been shown to effectively address challenging behaviour, improve communication and increase positive outcomes related to social learning, peer relationships and academic results (Walker & Snell, 2013; Hines & Simonsen, 2008; Ganz, Parker & Benson, 2009; Lerna et al., 2012).
FURTHER INFO:
Take a look at our page on visuals (where you can get LOADS of free visuals) here.
Relaxation – What is the evidence?
RELAXATION
This month the review of the evidence is all about something to follow on from the bullying update – Relaxation. You can check out all things Mental Health on our page here!
RESEARCH
All children worry. Researchers have suggested that this worry is in part due to the fact that childhood is full of “firsts”, doing a lot of things for the first time (Hallowell, 2011). While some worries are
developmentally appropriate, for example being away from parents (relates to safety) or not having friends (relates to sociability), other anxieties get in the way of children functioning across different areas (school, home, etc.). As such, it is important for children to develop coping skills to manage their worries.
Broadly, stress management techniques have been found to be beneficial. In particular, there is evidence to indicate that strategies like yoga, breathing techniques, relaxation response techniques, and sensorimotor awareness activities can improve psychosocial well-being, self-regulations, self-esteem, behaviour and cognition (Dacey, Mack & Fiore, 2016; Gard, et al. 2012; Bothe, Grignon & Olness, 2014).
Below is a list of stress management techniques children can try:
Physical Strategies
· Tense and release muscles / guided muscle relaxation
· Massage
· Exercise
· Playing sport
· Yoga
Psychological Strategies
· Grounding
· Visualisation
· Coping statements
· Meditation
· Distraction
· Redirection
FURTHER READING:
Take a look at Relax Kids here. They have a great portal that you can access for learning about and teaching relaxation.
REFERENCES:
Bothe, D. A., Grignon, J. B., & Olness, K. N. (2014). The effects of a stress management intervention in elementary school children. Journal of Developmental & Behavioral Pediatrics, 35(1), 62-67.
Broderick, P., & Metz, S., (2009). Learning to BREATHE: A pilot trial of a mindfulness curriculum for adolescents. Advances in School Mental Health Promotion, 2(1), 35-46.
Dacey, J. S., Mack, M. D. & Fiore, L. B. (2016). Your Anxious Child: How Parents and Teachers Can Relieve Anxiety in Children (2nd Ed.). New York, ny; John Wiley & Sons, Ltd.
Gard, T., Brach, N., Holzel, B.K., Noggle, J.J., Conboy. L.A., & Lazar, S.W. (2012). Effects of a yoga based intervention for young adults on quality of life and perceived stress: The potential mediating roles of mindfulness and self-compassion. Journal of Positive Psychology, 7(3).
Hallowell, E. M. (2011). Worry: Hope and Help for a Common Condition. Random House Publishing Group
Singh, N. N., Lancioni, G. E., Winton, A. S., Karazsia, B. T., Myers, R. E., Latham, L. L., & Singh, J. (2014). Mindfulness-based positive behavior support (MBPBS) for mothers of adolescents with autism spectrum disorder: Effects on adolescents’ behavior and parental stress. Mindfulness, 5(6), 646-657.
Weaver, L. L., & Darragh, A. R. (2015). Systematic Review of Yoga Interventions for Anxiety Reduction Among Children and Adolescents. American Journal of Occupational Therapy, 69(6), 6906180070p1-6906180070p9.
Children with additional needs accessing hospitals – What does the evidence say?
WHAT DOES THE EVIDENCE SAY? Children with additional needs accessing hospital and emergency departments.
Through each developmental stage, children interpret, comprehend, and process the world in a variety of different ways. Children and adolescents having to be treated in hospital, especially children with additional needs, can find the experience of being poked and prodded by strangers quite confronting. Additionally, it can be developmentally appropriate for children to experience anxiety related to separation or body integrity whilst in hospital. As such there has been a relatively recent push by medical and allied health professionals to take into account the psychological needs of children on an individual and age-appropriate basis. In particular, the need for a calming and minimally disruptive environment that reduces anxiety and allays fear.
Research indicates that in addition to taking into consideration a child’s age, developmental level and temperament when children are hospitalised, there are a number of other techniques that can be used to promote a minimally disruptive environment. These can include:
· Giving the child developmentally appropriate information regarding the medical procedure
· Encouraging positive self-talk through coping statements (i.e. “I am strong”)
· Enhancing parent support
· Swaddling for infants
· Maintaining home routines while in hospital (i.e. wake and sleep times, school work, photos)
· Creating a predictable schedule for the child
· Providing choices for the child so as to create a level of control
· Incorporating consistent play into the child’s day
The available literature indicates that the benefits of professionals taking the time to incorporate these strategies range from decreasing anxiety, decreasing sensations of pain, and decreasing recovery periods.
FURTHER READING
Take a look out some of our resources on accessing the hospital/ ED here.
REFERENCES
DeMaso, D. R., & Snell, C. (2013, August). Promoting coping in children facing pediatric surgery. InSeminars in pediatric surgery (Vol. 22, No. 3, pp. 134-138). WB Saunders.
Moore, E. R., Bennett, K. L., Dietrich, M. S., & Wells, N. (2015). The Effect of Directed Medical Play on Young Children’s Pain and Distress During Burn Wound Care. Journal of Pediatric Health Care,29(3), 265-273.
Murtagh, J. E. (2006). Managing painful paediatric procedures. Australian Prescriber, 29(4), 94 – 96.
Okado, Y., Long, A. M., & Phipps, S. (2014). Association between parent and child distress and the moderating effects of life events in families with and without a history of pediatric cancer. Journal of pediatric psychology, jsu058.
Tobin, D. P. (2013). The Future of Child Life in Pediatrics and Its Implications for Health Care Professionals (Doctoral dissertation, Oakland University William Beaumont School of Medicine Oakland).